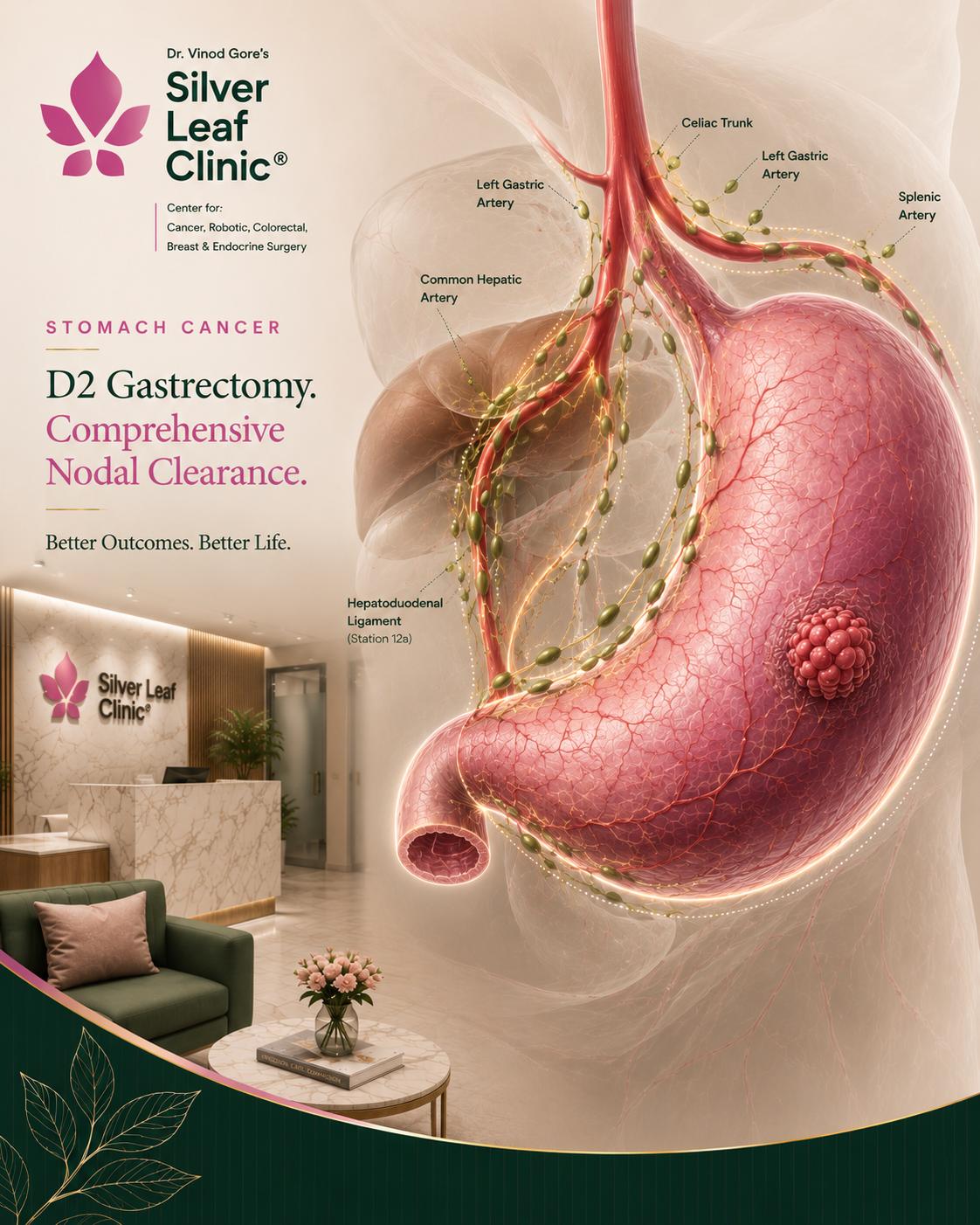
What is D2 lymphadenectomy and why does it matter?+
D2 means removing not just the lymph nodes immediately around the stomach (D1) but also those running along the major arteries that supply it. Because stomach cancer spreads to these nodes, a thorough D2 dissection lowers the chance of the cancer coming back. The Dutch trial showed D2 reduces recurrence and gastric-cancer death, which is why it is the world standard.
Is robotic gastrectomy better than laparoscopic or open surgery?+
All three can remove the cancer with a D2 dissection. Robotic surgery offers a magnified 3D view and wristed instruments that are particularly helpful for the delicate node clearance around the pancreas and major arteries — with less blood loss, faster recovery and the same cancer clearance. Open surgery remains appropriate for some very advanced tumours.
Will I need chemotherapy?+
Usually, yes, for tumours beyond the earliest stage. The FLOT regimen given before and after surgery improves cure rates. Targeted therapy (for HER2-positive cancers) or immunotherapy may be added in advanced disease.
Will my whole stomach be removed?+
Not always. For tumours in the lower stomach, only the lower part is removed (distal gastrectomy), preserving the upper stomach. Total gastrectomy — removing the whole stomach — is needed for upper, diffuse or extensive tumours.
How will I eat after the operation?+
You can eat normally again, but in smaller, more frequent meals, especially after a total gastrectomy. A dietitian supports you through the adjustment. After total gastrectomy you will need lifelong vitamin B12 injections, and iron levels are monitored.
Is stomach cancer caused by infection, and is it hereditary?+
Most stomach cancer is linked to long-standing Helicobacter pylori infection and to diet — treating the infection lowers risk. A small proportion is inherited (for example the CDH1 gene causing hereditary diffuse gastric cancer); families with a strong history should seek genetic counselling.