Indocyanine Green · Near-Infrared Imaging
ICG Fluorescence
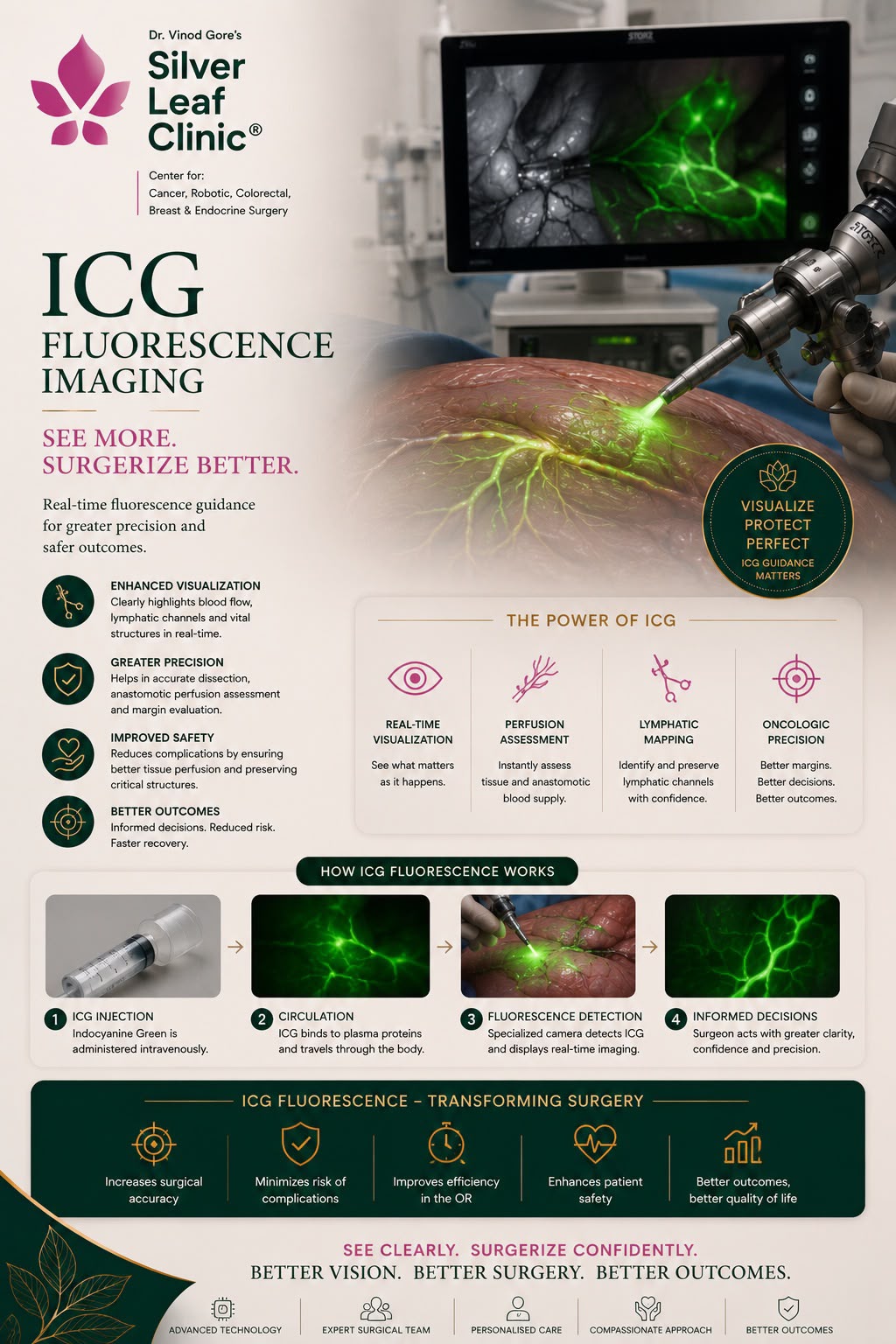
Seeing the Unseen in GI & Colorectal Surgery · Pune
ICG fluorescence lets the surgeon see things the naked eye cannot — whether bowel is getting a good blood supply, where a tumour ends, which lymph node drains it, and where delicate structures lie. A harmless green dye glows under near-infrared light, turning invisible anatomy into a live, glowing map during surgery. Dr. Vinod T. Gore uses ICG routinely — with the Stryker SPY system in open and laparoscopic surgery, and the built-in Firefly camera on the da Vinci Xi robot — to make cancer surgery safer and more precise.
Real-Time Imaging
Stryker SPY
da Vinci Firefly
Open · Lap · Robotic