Indications
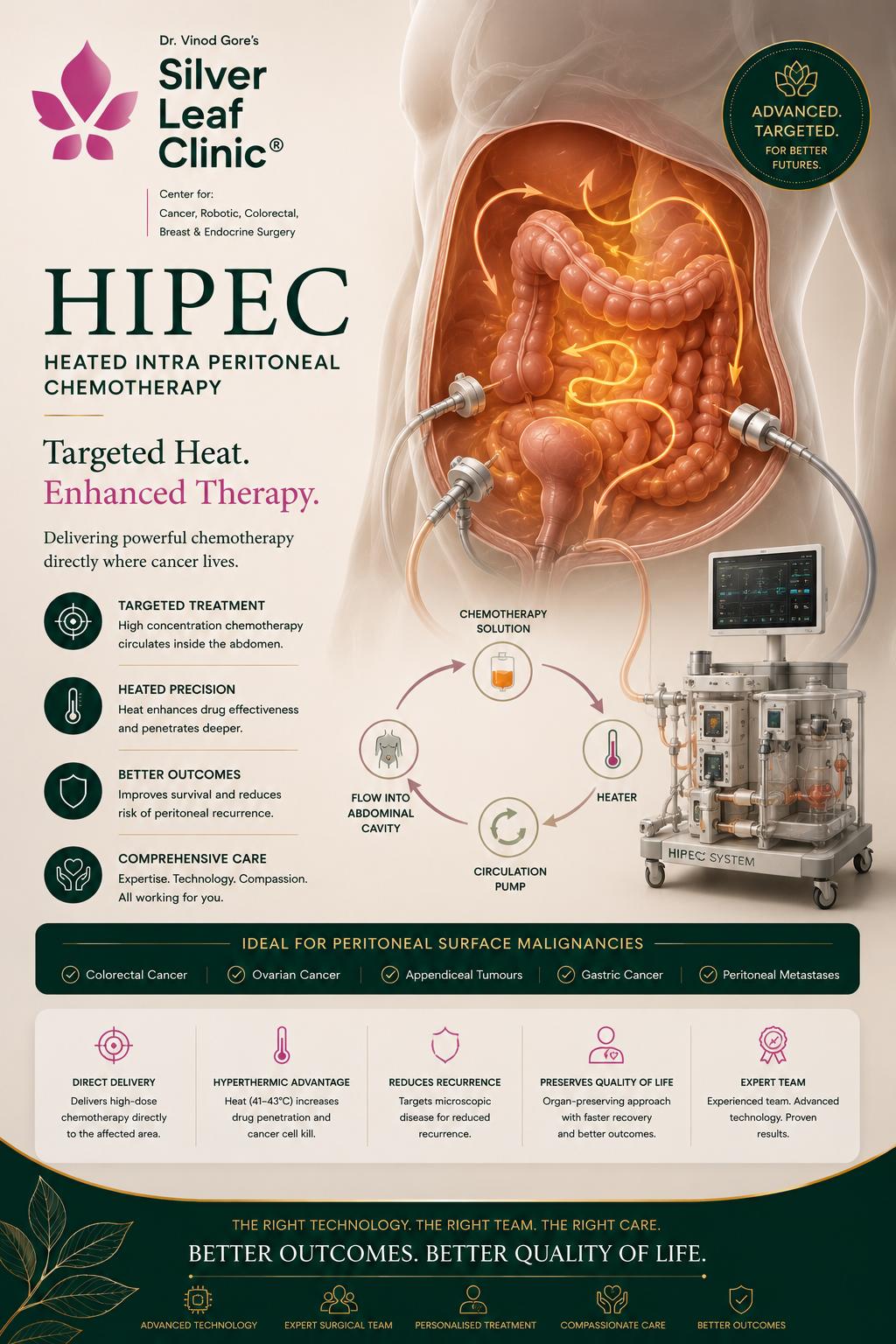
Who is HIPEC for?
HIPEC is not for every abdominal cancer. It is most effective when disease is confined to the peritoneal surfaces and can be completely removed. The strength of evidence differs by tumour type, so each indication is weighed individually at the tumour board.
Disease-wise indications, evidence & standard HIPEC regimen
| Cancer / Disease | Role of CRS + HIPEC | Evidence | Key trial | Typical HIPEC drug |
|---|
| Pseudomyxoma Peritonei |
Standard of care; potentially curative with complete cytoreduction |
Strong |
Large international registries |
Mitomycin-C |
Appendiceal cancer
(mucinous & non-mucinous) |
Well-established; resection of peritoneal disease + HIPEC |
Strong |
Registry & cohort data |
Mitomycin-C |
| Peritoneal mesothelioma |
Standard of care at specialist centres; markedly improves survival |
Strong |
Multi-institutional series |
Cisplatin ± Doxorubicin |
| Colorectal peritoneal metastases |
Complete cytoreduction is the key benefit; HIPEC used selectively |
Selective |
PRODIGE-7 (2021) |
Oxaliplatin / Mitomycin-C |
| Ovarian cancer (interval, selected) |
Survival benefit when added to interval debulking after chemotherapy |
Supported |
van Driel, NEJM 2018 |
Cisplatin |
| Gastric cancer (selected) |
Limited peritoneal disease / selected cases; evidence still evolving |
Investigational |
GASTRIPEC; ongoing trials |
Mitomycin-C / Cisplatin |
Drugs and timing are individualised per tumour type, prior chemotherapy and renal function, and decided at the multidisciplinary tumour board. Perfusion is typically delivered at 41–43 °C for 30–90 minutes.
When HIPEC is not advised
HIPEC is generally not suitable when disease is too extensive to remove completely (very high PCI), when cancer has spread outside the abdomen (liver, lungs, distant nodes), or when a patient is not fit enough for a long operation. Recognising this honestly is part of good care — offering HIPEC where it cannot help does harm. A frank selection assessment protects you.
The Operation
How CRS + HIPEC is performed
This is one of the longest and most complex operations in surgical oncology — often 8 to 12 hours. It is delivered by an experienced team with specialist anaesthesia and critical-care support.
Step 1
Exploration & PCI scoring
The abdomen is opened and fully assessed. The Peritoneal Cancer Index (PCI, 0–39) measures how much disease is present across 13 regions — confirming whether complete removal is achievable.
Step 2
Cytoreductive surgery
Every visible tumour deposit is removed — stripping peritoneal surfaces (peritonectomy) and, where needed, resecting involved bowel, omentum, spleen or other organs. The aim is CC-0.
Step 3
Heated chemotherapy perfusion
Catheters circulate chemotherapy heated to 41–43 °C throughout the abdomen for 30–90 minutes, reaching every surface. The drug and timing depend on the cancer type.
Step 4
Reconstruction & recovery
Any bowel joins are completed, the abdomen is closed, and recovery begins in intensive care. A hospital stay of around two weeks is usual.
PCI score (0–39)
CC score (CC-0 / CC-1)
Peritonectomy
Mitomycin-C / Oxaliplatin / Cisplatin
41–43 °C perfusion
ICU recovery
Peritoneal Cancer Index (PCI) — 13 regions × lesion size
| Region (0–12) | Area assessed | Lesion Size score | Meaning |
|---|
| 0–8 | Central, right/left upper & lower, flanks, epigastrium, pelvis | LS 0 | No tumour visible |
| 9–12 | Upper & lower jejunum, upper & lower ileum | LS 1 | Nodules up to 0.5 cm |
| Each of the 13 regions is scored LS 0–3 → | LS 2 | Nodules 0.5–5 cm |
| Total PCI = sum of all regions (0–39) | LS 3 | Nodules > 5 cm or confluent |
Reading the total (Sugarbaker): lower PCI predicts a higher chance of complete cytoreduction and better outcomes. As a general guide, colorectal peritoneal disease is most favourable at PCI < 20 (and especially < 12); pseudomyxoma can be resected at much higher indices. PCI is an aid to judgement, weighed with disease type, location and fitness — not a rigid cut-off.
Completeness of Cytoreduction (CC) score
| Score | Residual disease after surgery | Prognostic meaning |
|---|
| CC-0 | No visible residual tumour | Optimal — the goal |
| CC-1 | Residual nodules ≤ 2.5 mm | Complete — HIPEC can penetrate |
| CC-2 | Residual nodules 2.5 mm – 2.5 cm | Incomplete |
| CC-3 | Residual nodules > 2.5 cm | Incomplete |
Why CC matters most: heated chemotherapy penetrates only 2–3 mm, so it can only sterilise microscopic disease. The survival benefit of the whole operation depends on achieving CC-0 or CC-1. If complete cytoreduction cannot be achieved, HIPEC offers little — which is why honest patient selection comes first.
HIPEC surgery Pune · HIPEC India · cytoreductive surgery · CRS HIPEC · peritoneal cancer treatment Pune · peritoneal carcinomatosis · pseudomyxoma peritonei · PMP treatment · appendiceal cancer surgery · peritoneal mesothelioma · Sugarbaker procedure · heated chemotherapy surgery · best HIPEC centre western India