Intestinal NET · Small Bowel · Carcinoid
Neuroendocrine Tumour Treatment
Intestinal NETs · DOTATATE · PRRT · Surgery · Pune
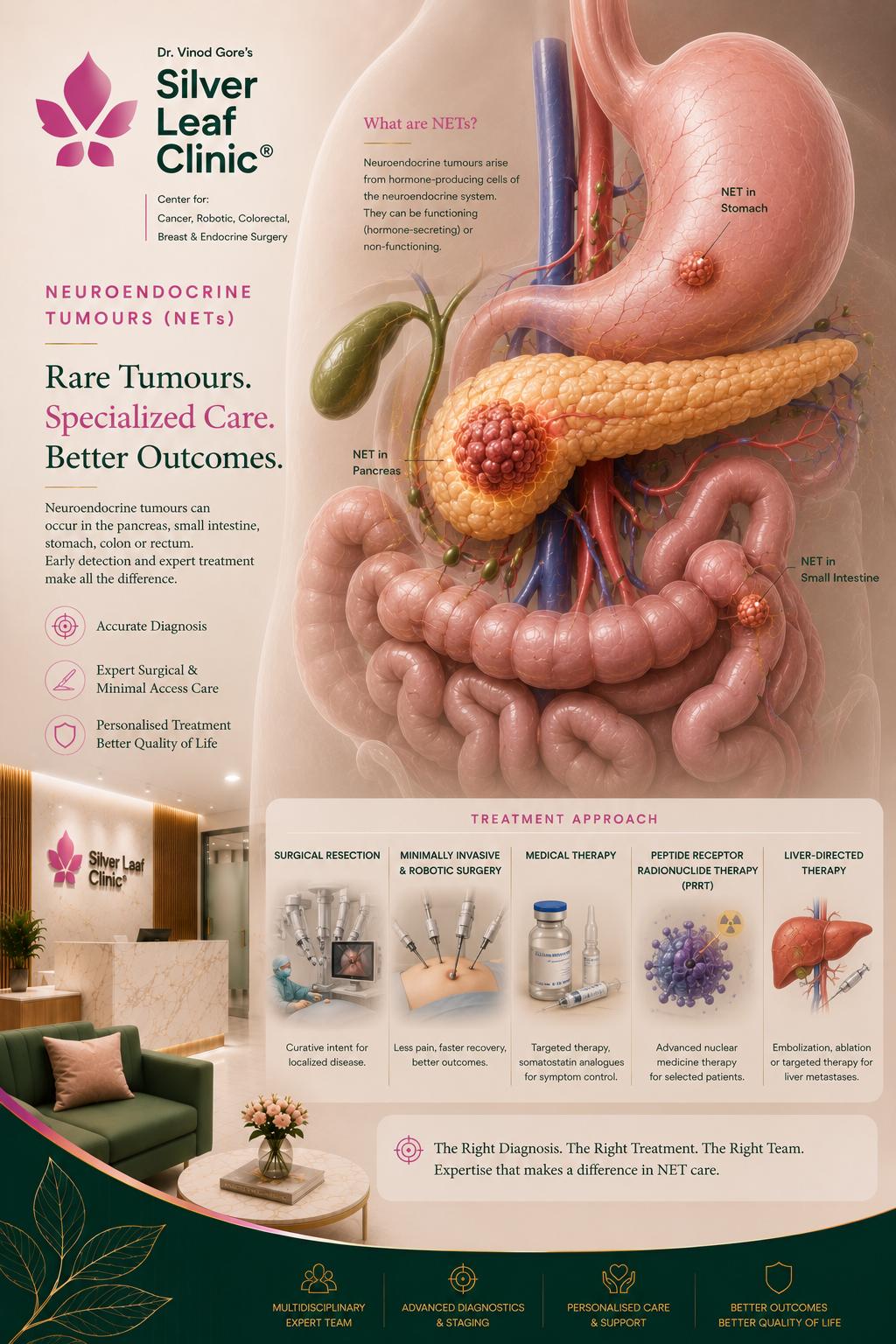
Neuroendocrine tumours of the gut grow slowly but behave very differently from common bowel cancer — so they need a different team and a different plan. Dr. Vinod T. Gore manages intestinal (small bowel and other GI) NETs end to end: precise grading and staging, Ga-68 DOTATATE PET-CT, somatostatin analogues and PRRT where appropriate, and surgery when resection offers the best control or cure.
Ga-68 DOTATATE PET-CT
WHO Grading G1–G3
Somatostatin Analogues · PRRT
Surgical Resection