Why is robotic surgery especially good for esophageal cancer?+
Because open esophagectomy requires opening the chest and spreading the ribs, lung complications such as pneumonia are common and serious. Robotic surgery (RAMIE) performs the same operation through small ports with a magnified 3D view. The randomised ROBOT trial showed this roughly halved serious lung and heart complications, with less blood loss and faster recovery — and the same cancer clearance.
Will I need chemotherapy or radiotherapy before surgery?+
Usually, yes, for locally-advanced tumours. The CROSS regimen (chemotherapy with radiotherapy before surgery) improves survival for both squamous and adenocarcinoma. For junctional adenocarcinoma, perioperative chemotherapy (FLOT) is an alternative. Upper or neck squamous cancers may be treated with chemoradiation alone.
What is the difference between squamous cell cancer and adenocarcinoma?+
Squamous cell carcinoma usually affects the upper/middle esophagus and is linked to smoking, alcohol and hot drinks; it is very sensitive to radiotherapy. Adenocarcinoma affects the lower esophagus and the junction with the stomach and is linked to reflux, Barrett’s and obesity. The type changes the treatment plan and the type of operation.
Can esophageal cancer be cured without surgery?+
Sometimes — particularly squamous cell cancers of the upper esophagus or neck, which can be cured by definitive chemoradiation alone. The decision is individual and made at the tumour board.
What is the difference between Ivor Lewis and McKeown surgery?+
Ivor Lewis uses an abdominal and a chest approach, with the join made in the chest — suited to lower and junctional tumours. McKeown adds a neck incision, with the join made in the neck — suited to middle and upper tumours and allowing three-field lymph node removal.
What is two-field versus three-field lymphadenectomy?+
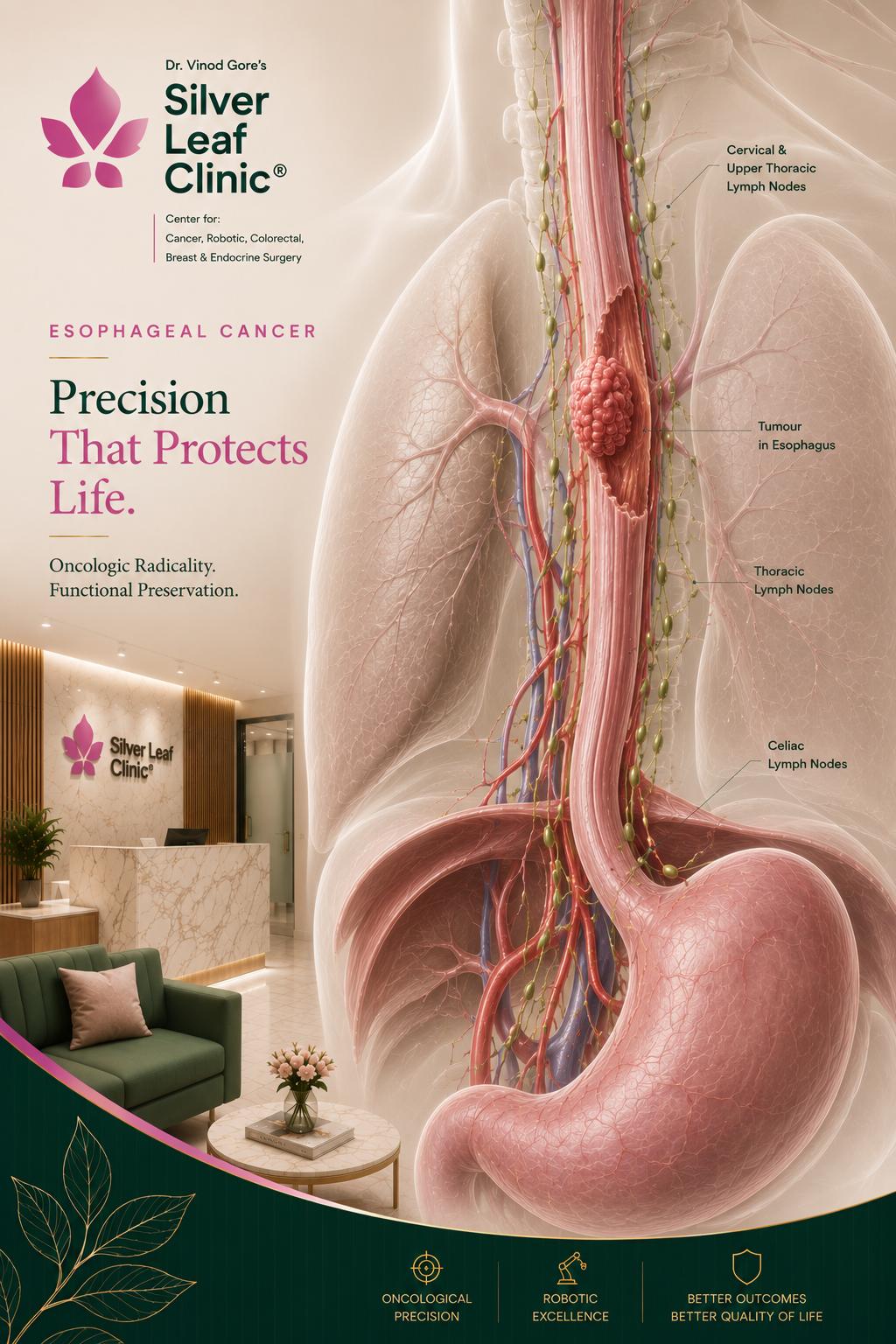
Two-field removes lymph nodes in the abdomen and chest; three-field also removes neck (cervical) nodes. Three-field is considered mainly for upper and middle squamous cancers, where neck nodes are more often involved.
How is recovery and eating after an esophagectomy?+
Recovery is supported with early mobilisation and a staged return to eating, often starting with small, frequent meals. With robotic surgery, pain and lung complications are reduced, which helps a smoother recovery. The team and a dietitian support you throughout.