Can pancreatic cancer be operated on and cured?+
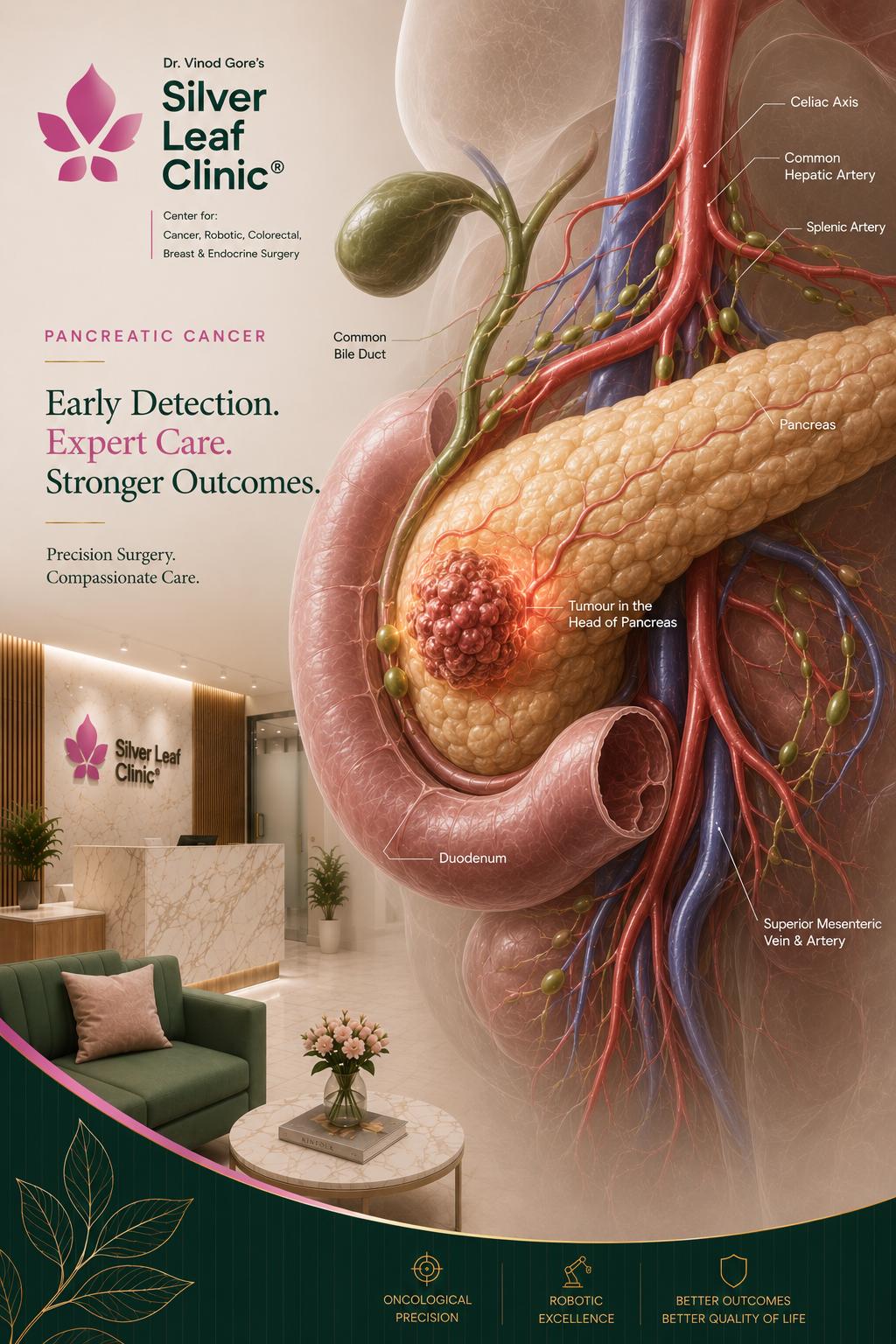
Surgery offers the only chance of cure, but it is only possible when the tumour can be removed completely — which depends on its relationship to the major blood vessels (resectability). Some borderline tumours can be made operable with chemotherapy first. An experienced pancreatic surgeon should always assess the scans, as tumours sometimes judged inoperable elsewhere can be removed in expert centres.
What is the Whipple procedure?+
The Whipple (pancreaticoduodenectomy) removes the head of the pancreas along with the duodenum, gallbladder and lower bile duct, then reconnects the remaining pancreas, bile duct and stomach to the bowel. It is the main curative operation for cancers of the pancreatic head, and Dr. Gore performs it both robotically and open.
Is robotic Whipple better than open surgery?+
In experienced hands, robotic Whipple offers less blood loss, fewer wound infections and a shorter hospital stay, with the same cancer clearance and margins as open surgery. It is one of the most advanced robotic operations and should only be done by surgeons with specific training and high volume.
Will I need chemotherapy before or after surgery?+
Usually both are considered. Chemotherapy before surgery (neoadjuvant) is used for borderline tumours to improve the chance of complete removal. Chemotherapy after surgery (adjuvant), such as modified FOLFIRINOX, significantly improves survival and is a crucial part of treatment.
How will I live after pancreatic surgery?+
Most patients return to a good quality of life. You may need pancreatic enzyme capsules with meals to digest food, and blood sugars are monitored (insulin is always needed after total pancreatectomy). A dietitian supports your recovery and nutrition throughout.
Why does choosing an experienced surgeon matter so much?+
Pancreatic surgery is technically complex and carries real risks. Studies consistently show that outcomes — including safety and survival — are significantly better when the operation is done by a high-volume surgeon in a high-volume centre. Experience is one of the most important factors in a good result.